Whether you’re in medical school lectures, clerkships, internal medicine residency, or studying for a board exam, it’s one of the most frustrating Internal Medicine topics to master. We’re of course talking about cardiac murmurs. Understanding them requires a consideration of cardiovascular physiology.
Internal Medicine Board Review: Cardiac Murmurs
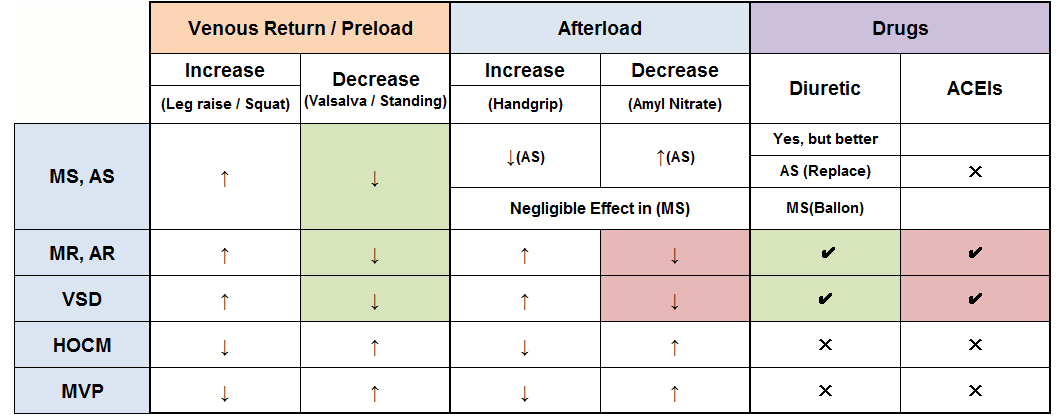
↑=↑ Murmur Intensity
↓=↓Murmur Intensity
↓ with Valsalva = ✔ Diuretics
↓ with Amyl Nitrate = ✔ ACEIs
MS= Mitral Stenosis AS= Aortic Stenosis MR= Mitral Regurgitation AR= Aortic Regurgitation VSD= Ventricular Septal defect HOCM= Hypertrophic Obstructive Cardiomyopathy MVP= Mitral Valve Prolapse
Understanding Murmurs and Maneuvers: Understanding heart auscultation and specifically some effects of various maneuvers on murmurs plays an important role in the cardiology section on any medical exam board (USMLE Step 2 CK and 3), as well as the Internal Medicine boards.
Common Murmurs:
| Systolic | Diastolic |
|---|
| Aortic Stenosis | Aortic Regurgitation |
| Mitral Regurgitation | Mitral Stenosis |
| MVP | |
| HOCM | |
An important concept to keep in mind is that maneuvers affect the volume of blood entering the heart chambers.
- Right-sided murmurs are increased with inhalation
- Left-sided murmurs are increased with exhalation
VENOUS RETURN / PRELOAD:
What increases venous return to the heart / Preload?
- Squatting
- Lifting the legs
What decreases venous return to the heart / Preload?
Squatting → Squeezes blood up into the heart → ↑Blood return to the heart.
Valsalva → ↑Intrathoracic pressure → ↓ Blood return to the heart. We can clearly observe in the table that MS, AS, MR, AR and VSD become louder with leg raising and squatting, except HOCM and MVP, which become softer with these maneuvers. On the other hand, MS, AS, MR, AR and VSD become softer with valsalva and standing, except HOCM and MVP, which become louder with such maneuvers.
AFTERLOAD:
What increases afterload?
What decreases afterload?
Handgrip → Contract arms muscle → Compresses arteries of the arm
Amyl Nitrate (Vasodilator) → Dilate peripheral arteries
As we can see in the table, handgrip softens the aortic stenosis murmur by preventing blood leaving the ventricles. In other words, if the afterload goes up, blood cannot be ejected from the left ventricles, and the aortic stenosis murmur will soften.
In Amyl nitrate, if the afterload goes down, blood can be easily ejected from the left ventricles, and finally worsening or making it louder.
An important point to mention is that handgrip and Amyl nitrate have a negligible effect on mitral stenosis since both maneuvers do not affect ventricular filling which is important in such murmurs.
Aortic and mitral regurgitation are worsen or louder by handgrip because this pushes blood backward into the heart. The same rule apply for VSD, since more blood goes from the left to the right and making it louder.But since Amyl nitrate has the opposite result of hangrip, then this improves both aortic and mitral regurgitation.
On the other hand, while handgrip improves or soften the MVP and HOCM murmurs due to a large left ventricle caused by the increased afterload, Amyl Nitrate will result in an opposite effect which appear as an increased ventricular emptying due to a decreased afterload that ultimately worsen the obstruction and makes the murmur louder.
DRUGS:
Based on the table above, we can observe that mitral and aortic regurgitation can be treated with vasodilators, like ACEi, and ARBs.
ACE inhibitors basically functions as the opposite of handgrip, by decreasing afterload which at the same time increases the forward flow of blood out of the left ventricle. In some cases when the medical therapy is not enough, then valve replacement is the best option.
On the other hand, mitral and aortic stenosis are appropriately treated with surgery. Whereas mitral stenosis is treated with balloon valvuloplasty (or valve replacement when valvuloplasty is not an option depending on certain valve characteristics), aortic stenosis is best treated with valve replacement.
Note: Even though diuretics can decrease pulmonary vascular congestion in either mitral or aortic stenosis, they are not as effective as balloon valvuloplasty or valvular replacement. Also important to mention, is that ACE inhibitors have scant effect on mitral stenosis.
An important concept that can help us to remember the uses of diuretics and ACEIs is as follows:
- If valsalva improves the murmur, diuretics can be used.
- If Amyl nitrate improves the murmurs, ACEIs can be used.