Oncology is an essential part of the Internal Medicine Medical Clerkship and ABIM Board exam. According to the ABIM exam blueprint, questions testing Oncology topics comprise ~7% of the exam. Initially, oncology seems like a very difficult subject given how the treatment regimens of the many types of carcinomas are ever-changing. However, realize that Internal Medicine exams are focused on the basics of the different malignancies. These 8 pearls will get you off to a good start for identifying
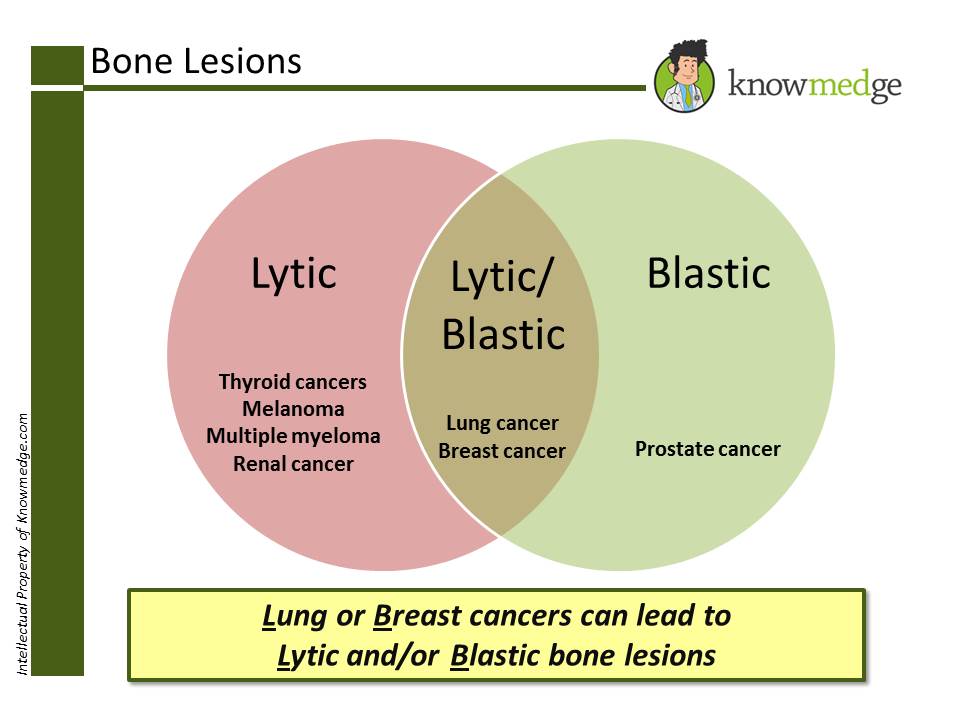
1. Which cancers correspond to lytic bone lesions? Blastic? Lytic or Blastic?
1. Which cancers correspond to lytic bone lesions? Blastic? Lytic or Blastic?
- Lytic bone lesions
- Melanoma
- Multiple Myeloma
- Renal cell cancer
- Thyroid cancer
- Blastic bone lesions
- Prostate cancer
- Lytic or blastic lesion
- Lung cancer
- Breast cancer
Click on image to enlarge
2. Which paraneoplastic syndrome goes with which cancer?
Click on image to enlarge
3. Know these high-yield Breast Cancer facts for the ABIM and IM shelf exams- If the lesion is >1cm OR the patient has lymph node involvement → chemotherapy will be part of the treatment protocol.
- If sentinel node biopsy is negative → no further lymph node biopsy is required
- If the patient’s breast cancer is ER/PR (+) and patient is pre-menopausal →Tamoxifen is given X 5 years
- If the patient’s breast cancer is ER/PR (+) and is post-menopausal → Aromatase inhibitors (eg. Anastrozole) is given
- If the patient’s breast cancer is HER2/neu (+)→ Trastuzumab is given →can cause CHF →check echocardiogram to assess left ventricular function
- Triple negative breast cancer (ER negative, PR negative, HER2/neu negative) have the worst prognosis
- t (14,18) → Follicular Lymphoma
- t (8,14) → Burkitt’s Lymphoma
- t (9,22) → Known as Philadelphia Chromosome (BCR-ABL) gene fusion → good prognosis in CML patients and bad prognosis in ALL patients
- t (15,17) → Acute promyelogenous Leukemia (M3) → good prognosis → Treatment is with All-Trans Retinoic Acid (ATRA)
- t (11,14) →Mantle cell Lymphoma → highly aggressive form of Non-Hodgkin’s Lymphoma → cyclin D1 oncogene is overexpressed → treat with R-CHOP
- Seminomas are Radiation sensitive and usually have a normal AFP and HCG level
- Non-Seminomas (eg, yolk sac tumor, embryonal carcinoma, teratoma, choriocarcinoma) are radiation resistant and usually have elevated AFP and HCG level

Click on image to enlarge
6. High-yield facts about Colon Cancer for the ABIM and IM Shelf Exam- If cancer invades mucosa or sub-mucosa → colon resection is required
- If cancer invades muscularis propria, serosa, or has LN involvement →colon resection is required +chemotherapy (usually FOLFOX) +/- Irinotecan. FOLFOX is 5 flurouracil, Oxaliplatin, and Leucovorin
- Most common area of metastasis for colon cancer is the liver
- If solitary liver lesion →resection of liver can be performed
- If multiple liver lesions → poor prognosis and survival rate is low
- Neck and facial swelling
- Dyspnea
- Cough
- Physical examination will show distended jugular veins
- Chest x-ray may reveal mediastinal widening or right hilar mas
- Most common cause is lung cancer (particularly small cell lung cancer). Malignant lymphoma is also a well-known cause of superior vena cava syndrome
- Management obviously requires treatment of the underlying malignancy but symptomatic measures such as diuretics and elevation of the bed usually suffice
- Most common cancers that cause spinal cord compression are: Lung cancer, breast cancer, prostate cancer, multiple myeloma, and lymphoma
- Back pain is the most commonly presenting symptom. Other concerning symptoms include muscle weakness, numbness/tingling, cauda equina syndrome, and loss of bowel or bladder control
- Diagnosis is required promptly to prevent further neurological deterioration and an MRI OF THE ENTIRE SPINE IS REQUIRED FOR DIAGNOSIS
- Management for spinal cord compression is with Dexamethasone 10 mg IV X 1 dose, followed by Dexamethasone 4 mg IV every 6 hours.
- Radiation therapy can help in shrinking the tumor; however, recent studies indicate that surgical decompression is superior to RT. Therefore, an immediate neurosurgical consultation is required when this condition is suspected or diagnosed.
- Intracellular contents leak out into the bloodstream.
- Although this condition can occur with any malignancy, it is more common in aggressive lymphomas and hematological malignancies.
- Hyperkalemia, Hyperuricemia, Hyperphosphatemia, Acute renal failure, and hypocalcemia are often seen in patients with tumor lysis syndrome
- Management of tumor lysis syndrome requires electrolyte abnormality correction, aggressive hydration, and allopurinol
No comments:
Post a Comment